Atherosclerosis & Vascular Disease +
Familial Hypercholesterolemia (FH)
Understanding the hidden damage of inherited high cholesterol and how it accelerates artery disease
Atherosclerosis & Vascular Disease: The Hidden Damage of Familial Hypercholesterolemia
Most people think of heart disease as something that happens later in life.
But for individuals with Familial Hypercholesterolemia (FH), artery damage can begin silently — sometimes in childhood.
FH causes lifelong elevation of LDL ("bad") cholesterol. Over time, this excess LDL injures blood vessels, accelerates plaque formation, and dramatically increases the risk of heart attack and stroke.
To understand why early diagnosis of FH is so critical, we must first understand how atherosclerosis and vascular disease develop.
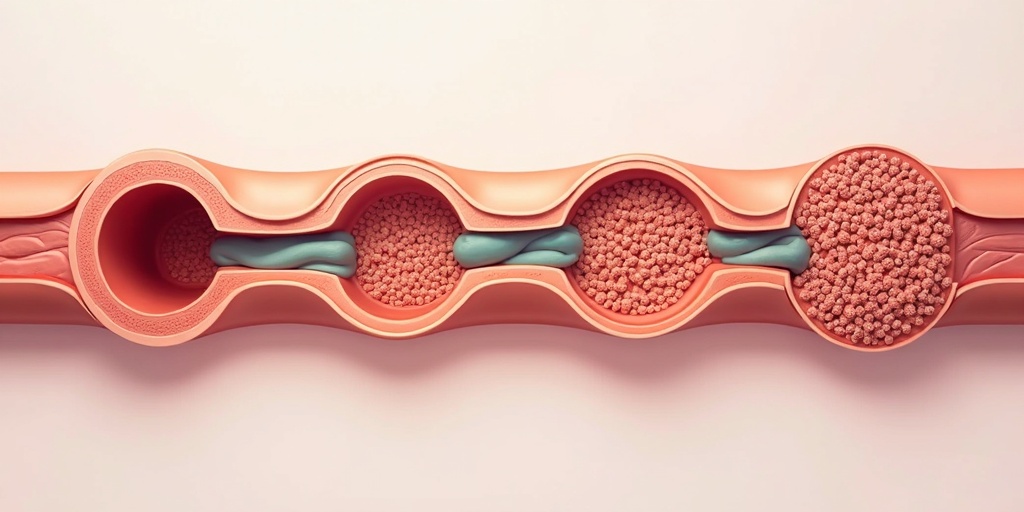
What Is Atherosclerosis?
Atherosclerosis is the buildup of cholesterol-rich plaque inside arteries. These plaques narrow vessels, reduce blood flow, and can rupture — causing heart attacks or strokes.
In FH, this process happens earlier, faster, and more aggressively.
How Atherosclerosis Develops in FH
Six critical stages of vascular disease in Familial Hypercholesterolemia patients
Premature Atherosclerosis
"Premature" means artery disease occurring decades earlier than expected. In untreated FH: Plaque can begin forming in teenage years, heart disease may appear in the 30s or 40s, and severe cases can affect children. Because LDL levels are elevated from birth, arteries are exposed to continuous damage over time — a concept known as lifetime LDL burden.
Endothelial Dysfunction
The endothelium is the thin inner lining of blood vessels. Healthy endothelium regulates blood flow, prevents clotting, and controls inflammation. High LDL in FH injures this lining early. Once damaged, the vessel becomes more permeable to cholesterol and inflammatory cells — setting the stage for plaque formation. Endothelial dysfunction is often the first detectable step toward vascular disease.
Arterial Plaque Formation
When LDL particles penetrate the damaged vessel wall: They become trapped, immune cells attempt to clear them, and foam cells accumulate. This leads to fatty streaks that gradually evolve into fibrous plaques. In FH, plaque accumulation is more extensive and often affects multiple arteries simultaneously.
Oxidized LDL Injury
LDL particles can undergo chemical modification inside the artery wall, becoming oxidized LDL. Oxidized LDL triggers strong inflammatory responses, is highly toxic to vessel lining, and accelerates plaque growth. Because LDL levels are chronically elevated in FH, the amount of oxidized LDL is also increased — compounding vascular injury.
Vascular Inflammation
Atherosclerosis is not just a cholesterol problem — it is an inflammatory disease. Persistent LDL exposure leads to: Activation of immune cells, release of inflammatory cytokines, and chronic vascular irritation. Inflammation weakens plaque structure and increases risk of rupture.
Plaque Instability
Not all plaques are equally dangerous. Stable plaques grow slowly and cause predictable symptoms. Unstable plaques have thin fibrous caps, are prone to rupture, and trigger sudden clot formation. In FH, the combination of high LDL and inflammation increases the risk of plaque instability — which can lead to sudden heart attack or stroke.
Vascular Disease Beyond the Heart
FH affects arteries throughout the body — not just coronary arteries
Carotid Intima-Media Thickening
The carotid arteries in the neck supply blood to the brain. In FH: Ultrasound often shows thickening of the carotid artery wall. This is an early marker of atherosclerosis. Carotid intima-media thickening can be detected years before symptoms appear, offering a window for early intervention.
Coronary Artery Calcification
As plaques mature, calcium deposits form inside artery walls. Coronary artery calcium (CAC) scoring: Measures calcified plaque burden and predicts heart attack risk. In FH patients, CAC scores are often elevated at younger ages, reflecting accelerated plaque progression.
Peripheral Artery Disease (PAD)
Atherosclerosis can also affect arteries in the legs. Peripheral artery disease may cause: Leg pain during walking (claudication), slow wound healing, and reduced mobility. In severe FH, systemic plaque burden increases the likelihood of PAD.
Cerebrovascular Disease
When plaques affect arteries supplying the brain, the risk of stroke increases. Cerebrovascular complications include: Transient ischemic attacks (mini-strokes), ischemic stroke, and cognitive impairment. Elevated LDL and Lipoprotein(a), often present in FH, further increase stroke risk.
Why Familial Hypercholesterolemia Changes the Timeline
In the general population, atherosclerosis develops gradually with aging and lifestyle factors.
In FH:
- Elevated LDL is present from birth
- Damage accumulates every year
- Arteries age faster than the person
This accelerated timeline explains why many individuals with FH experience vascular disease decades earlier than expected.
The Silent Nature of Vascular Disease
One of the greatest dangers of FH is that vascular injury may remain silent for years.
There may be:
- No chest pain
- No warning signs
- No visible symptoms
Until suddenly — a heart attack or stroke occurs.
Early screening can identify risk long before symptoms appear.
The Power of Early Detection
When FH is diagnosed early:
- Aggressive LDL lowering can slow plaque formation
- Inflammation decreases
- Plaque stabilization improves
- Risk of heart attack and stroke drops dramatically
Modern therapies can reduce LDL by 50–70% or more — transforming long-term outcomes.
Raising Awareness
People worldwide have FH
Remain undiagnosed
If you or a family member has:
- LDL cholesterol above 190 mg/dL
- Early heart disease in the family
- Stroke or vascular disease at a young age
Ask about FH screening.
Because when it comes to atherosclerosis, timing is everything.
Final Takeaway
Atherosclerosis and vascular disease are not sudden events — they are long, silent processes.
In Familial Hypercholesterolemia, that process begins early and progresses faster.
The good news?
When identified early, vascular damage can be slowed, stabilized, and in many cases prevented.
Awareness
The first step
Testing
The second step
Early Treatment
The life-saving difference
Awareness of FH does not just reduce cholesterol — it protects arteries for a lifetime.
Critical Statistics
When plaque formation can begin in FH
Years earlier atherosclerosis develops in FH
Arteries often affected simultaneously in FH
Early Detection Saves Lives
If you have a family history of early heart disease or high cholesterol, don't wait for symptoms. Early screening and aggressive LDL control can prevent these devastating outcomes.