Coronary Artery Disease (CAD) +
Familial Hypercholesterolemia (FH)
Understanding the accelerated cardiovascular risk in patients with inherited high cholesterol
Coronary Artery Disease (CAD): The Silent Threat Behind Familial Hypercholesterolemia
Coronary Artery Disease (CAD) remains the leading cause of death worldwide. Yet for individuals living with Familial Hypercholesterolemia (FH), the risk is not just elevated — it is accelerated.
FH is a genetic condition that causes lifelong elevation of LDL ("bad") cholesterol. Over decades, this excess LDL quietly damages coronary arteries, often leading to heart disease 20–30 years earlier than in the general population.
Understanding how CAD develops — and how it presents — is critical to recognizing the life-saving importance of early FH diagnosis.
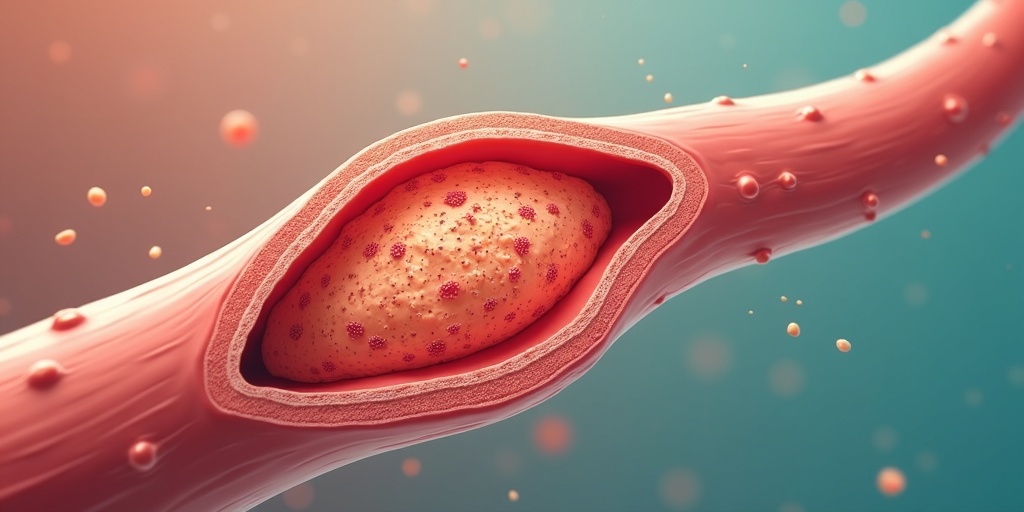
What is Coronary Artery Disease?
CAD occurs when cholesterol-rich plaque builds up inside the coronary arteries, narrowing blood flow to the heart muscle. In FH, this process begins early — sometimes even in childhood.
Over time, arteries stiffen, narrow, and become unstable. The result can range from chest discomfort to sudden cardiac death.
How CAD Manifests in Familial Hypercholesterolemia
Ten critical presentations of coronary artery disease in FH patients
Premature Coronary Artery Disease
"Premature" means occurring earlier than expected: Men <55 years and Women <65 years. In FH, heart attacks can occur in the 30s or 40s, and in severe cases even during teenage years. This early onset is one of the strongest clues pointing toward undiagnosed FH.
Stable Angina
Stable angina is chest pain that occurs predictably with exertion and improves with rest. It signals narrowed coronary arteries that cannot deliver enough oxygen during physical activity. In FH patients, stable angina may appear decades earlier than normal.
Unstable Angina
Unstable angina is more dangerous: occurs unpredictably, may happen at rest, and worsens over time. It often indicates a rupturing plaque — a warning sign that a heart attack may be imminent.
Acute Coronary Syndrome (ACS)
Acute Coronary Syndrome (ACS) is an umbrella term that includes unstable angina, non-ST elevation heart attack, and ST-elevation heart attack. ACS represents sudden blockage of coronary blood flow. FH patients are at significantly higher lifetime risk of ACS due to heavy LDL burden.
Myocardial Infarction (Heart Attack)
A myocardial infarction occurs when blood flow is completely blocked, causing heart muscle damage. In untreated FH: lifetime heart attack risk can exceed 50%, events often occur before age 50, and recurrence is common without aggressive therapy. Early LDL control dramatically reduces this risk.
Silent Ischemia
Not all heart damage causes pain. Silent ischemia refers to reduced blood flow without noticeable symptoms, often detected only on stress tests or imaging. This is especially concerning in FH because arterial damage may already be advanced before symptoms appear.
Multi-Vessel Coronary Disease
FH patients often develop plaque in multiple coronary arteries simultaneously. Multi-vessel disease increases surgical complexity, raises risk of heart failure, and often requires bypass surgery instead of stenting. This reflects the systemic nature of lifelong LDL exposure.
Left Main Coronary Artery Disease
The left main artery supplies a large portion of the heart. Blockage here is particularly dangerous: high risk of fatal heart attack and often requires urgent bypass surgery. Severe FH — especially in Homozygous Familial Hypercholesterolemia — significantly increases risk of early left main disease.
Recurrent Cardiac Events
Without aggressive LDL lowering, FH patients face repeat heart attacks, repeat stenting, and repeat hospitalizations. Even after one event, elevated LDL continues to fuel plaque progression unless treated intensively.
Sudden Cardiac Death
In some cases, the first symptom of FH-related CAD is sudden cardiac death due to fatal arrhythmias, massive heart attack, or complete coronary occlusion. This tragic outcome is often preventable with early screening and treatment.
Critical Statistics
Lifetime heart attack risk in untreated FH
Years earlier CAD develops in FH patients
Age when heart attacks often occur in FH
Why Familial Hypercholesterolemia Changes the Story
In most people, CAD develops gradually over decades due to lifestyle and aging.
In FH:
- Elevated LDL is present from birth
- Arteries accumulate damage year after year
- Risk compounds with time
This concept is called "cholesterol year burden" — the total lifetime exposure to LDL.
The longer LDL remains high, the greater the arterial injury.
The Good News: CAD in FH Is Preventable
When diagnosed early and treated aggressively:
- LDL can be reduced by 50–70% or more
- Heart attack risk drops by up to 80%
- Life expectancy approaches normal
Modern therapies — statins, ezetimibe, PCSK9 inhibitors, and in severe cases LDL apheresis — can dramatically alter outcomes.
The Awareness Gap
people has FH
remain undiagnosed
Many families discover FH only after a premature heart attack.
Recognizing CAD patterns — especially:
- Early heart attacks
- Multi-vessel disease at young age
- Family history of early cardiac death
— should immediately trigger evaluation for FH.
What You Can Do
If you or a family member has:
- LDL >190 mg/dL
- Heart attack before age 55
- Recurrent coronary disease
- Strong family history of early heart disease
Ask your physician about Familial Hypercholesterolemia testing.
Early diagnosis does not just save one life — it allows cascade screening of the entire family.
Final Takeaway
Coronary Artery Disease is devastating.
But when CAD is driven by Familial Hypercholesterolemia, it is also predictable and preventable.
Awareness is the first step
Testing is the second
Early treatment is the life-saving difference
If we identify FH early, we can stop premature heart disease before it begins.
Early Detection Saves Lives
If you have a family history of early heart disease or high cholesterol, don't wait for symptoms. Early screening and aggressive LDL control can prevent these devastating outcomes.